Fifty-two per cent of people who stay in psychotherapy for personality disorders no longer meet full diagnostic criteria after about 1.3 years of treatment. That is a real recovery signal, not just a temporary reduction in distress.
A college student who keeps replaying every awkward conversation, or a professional worn down by workplace stress, might first wonder if counselling can really help when patterns feel so deep. The evidence says structured therapy can, and it often helps people build resilience, steadier well-being, and more workable relationships over time.
Understanding Psychotherapy for Personality Disorders
Personality disorders involve long-standing patterns that affect how people think, feel, and relate to others. A person may notice the same painful loop showing up in relationships, at work, and at home, even while trying hard to respond differently.
What this means in plain language
Personality disorders are long-standing patterns of thinking, feeling, and relating that can become rigid and hard to shift. A simple way to understand this is that the mind has learned an old route for handling stress, and that route now causes more harm than help.
The pattern has become sticky, and psychotherapy for personality disorders aims to help people notice those patterns, understand them, and practise newer responses. That process is gradual, because the habits involved often developed over many years.

This is also where online assessments, including tools on platforms like DeTalks, can be useful as informational starting points. They can help someone reflect on symptoms, stress, relationships, or coping style, but they are not diagnostic labels.
Why therapy matters for daily life
People often come to counselling because daily life feels harder than it should. They may be dealing with anxiety, low mood, burnout, or repeated conflict, and they want a clearer way to understand what keeps getting in the way.
Therapy helps because it is more than a supportive conversation. It is a structured process that works on patterns over time, with attention to emotions, behaviour, relationships, and the person's sense of self.
Practical rule: if a pattern is affecting work, relationships, sleep, or self-worth, it deserves careful attention, not shame.
In India, this conversation often starts subtly, sometimes after family tension, exam pressure, or long-running workplace stress. The same ideas matter globally, because people everywhere need help that is respectful, evidence-based, and grounded in real life. The Still Water Wellness Group program is one example of how structured support can be organised around skill-building and steady practice.
Major Therapeutic Approaches Compared
A person seeking help for personality-related difficulties may arrive hoping for one clear answer. The evidence supports a more careful view. Structured psychotherapy can help, and different approaches suit different patterns of distress, relationships, and daily functioning, as shown in a systematic review.
How the main therapies differ
DBT, or dialectical behaviour therapy, is often used when emotions feel intense and relationships become turbulent. It focuses on emotion regulation, distress tolerance, and practical skills for getting through painful moments without making the situation worse.
MBT, or mentalisation-based therapy, helps a person notice mental states, their own and other people's. If someone keeps assuming the worst during a tense conversation, MBT gives them a way to slow down, reflect, and check their interpretation before reacting.
Schema therapy looks at older, deep-rooted patterns that may have started early in life. A person may recognise a familiar inner script, such as “I will be rejected,” and then work on replacing it with something less harsh and more realistic.
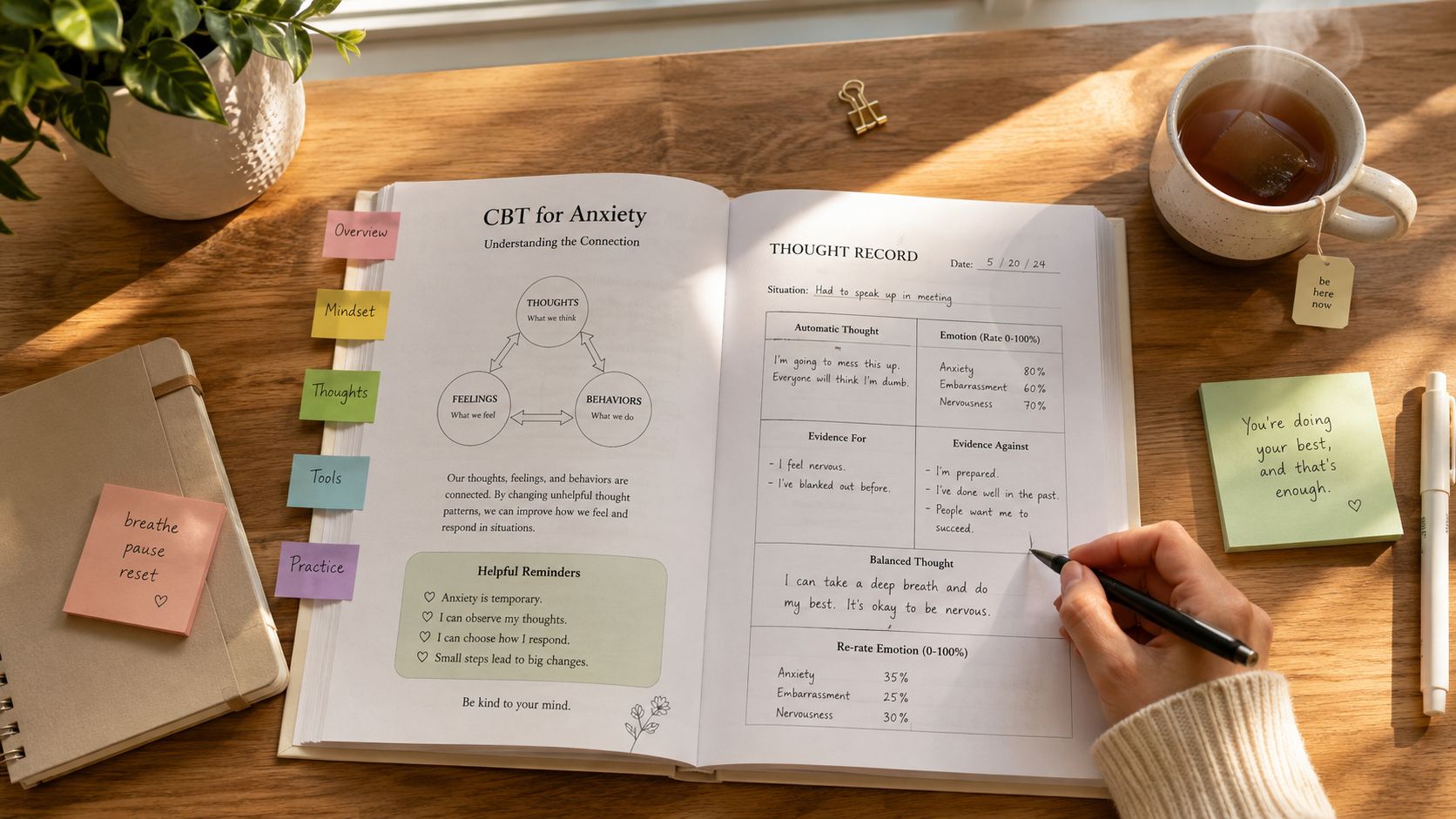
Cognitive-behavioural therapy helps people notice unhelpful thoughts and behaviours and try different responses. A concrete example might be pausing before sending a heated message, then testing a calmer reply instead.
| Therapy Approach | Core Focus | Best Suited For | Evidence Level |
|---|---|---|---|
| DBT | Emotional regulation and distress tolerance | Repeated crises, self-defeating coping, strong emotional swings | Limited but positive evidence, especially for borderline personality disorder (systematic review) |
| MBT | Understanding one's own and others' mental states | Misunderstandings in close relationships, quick shifts in trust | Limited but positive evidence (systematic review) |
| Schema therapy | Long-term relationship and self-patterns | Repeated relational pain, entrenched beliefs | Limited but positive evidence (systematic review) |
| Cognitive-behavioural therapy | Thoughts, behaviours, and coping habits | Practical change, coping skills, clearer routines | Supported in structured outpatient care (systematic review) |
For someone who wants a concrete example of skills-based care, the Still Water Wellness Group program shows how structured support can be organised around practice, feedback, and steady habits.
A useful comparison is that DBT often feels most concrete, MBT feels most reflective, schema therapy feels most pattern-based, and CBT feels most skills-focused. In India, that distinction can matter when someone is looking for therapy that fits family pressures, exam stress, or workplace strain, because the same therapy style does not suit every setting or every person.
The field still points to the same honest conclusion, no single branded model consistently dominates all others. What seems to matter most is structured, manualised treatment with good retention, rather than chasing a perfect label (systematic review).

What Treatment Goals and Structure Look Like
A person starting counselling often wants one simple thing, what will happen week to week. That question matters, because structure can make therapy feel safer and easier to use, especially when someone already feels overwhelmed.
How treatment is usually organised
For borderline personality disorder, one review notes that therapy often takes 6 to 12 months, and routine activity can support depression, stress, and anxiety. In practice, the length depends on goals, symptom burden, and how consistently someone can attend.
The work is usually collaborative. The therapist and client agree on targets such as fewer blow-ups, less avoidance, better sleep, or more stable relationships, then revisit those goals as life changes.
A common structure looks like this:
- Individual sessions: these are used to understand triggers, habits, and personal history in a private setting.
- Group formats: these can help with feedback, practise, and interpersonal skills in a real-time social setting.
- Manualised care: a clear framework helps both therapist and client know what the treatment is trying to do.
- Retention strategies: reminders, scheduling support, and a steady format matter because dropout is common.

A helpful way to picture the process is as a scaffold. The therapy itself is the work, but the structure holds that work in place while patterns are being understood and changed. For some people, that structure includes weekly one-to-one sessions. For others, it also includes a group where they can practise speaking, listening, and repairing misunderstandings in a safer setting.
That kind of clarity matters because recovery evidence is tied to treatment that people can stay with. A structured plan gives both sides something concrete to hold on to, especially when emotions run high or daily life in India, family expectations, commute time, exams, or shift work makes attendance difficult. The plan is not about sounding clinical. It is about making therapy usable in real life.
What to ask before you begin
Ask whether the therapist uses a structured approach, how progress is tracked, and whether they offer individual work, group work, or both. In India, that question matters because access to trained clinicians varies widely, so fit and consistency may matter more than a polished title.
Helpful question: “How do you handle it when therapy feels difficult or when I miss a session?”
That kind of question tells you something important. A good clinician will not promise ease, but they will explain the plan clearly and make space for honest discussion about barriers.
What to Expect in Therapy Sessions
Inside the therapy room, the work follows a clear structure that helps people notice change over time. A first session often begins with current stress, not with labels. Someone may talk about workplace stress, family arguments, panic, shutdown, or the feeling of being on edge all the time.
What happens inside the room
The therapist listens for patterns, not only for isolated events. They pay attention to what tends to happen before a reaction, what the reaction feels like, and what follows after it, because that sequence often shows where change can begin. It is a bit like watching how one loose step affects the rest of a staircase, once the pattern is visible, it becomes easier to work on it.
Progress is tracked in small ways. A person may notice fewer intense fights, less spiralling after a harsh email, or a steadier response to loneliness, and those shifts matter even when they feel modest. In everyday life, that can mean getting through a family conversation without shutting down, or pausing long enough to answer a message without feeling overwhelmed.
Therapy builds structured partnerships that support lasting change rather than offering quick fixes.
That structure also leaves room for compassion. People often come in with guilt, shame, or self-criticism, and therapy tends to work better when those feelings are handled with care rather than judgement. For many clients, that experience is new, because they have often been treated as difficult instead of as people trying to cope.
The process can feel harder before it feels easier. When old defences loosen, anxiety or sadness may rise for a while, and that does not mean treatment is failing. It often means the person is facing material that used to stay buried, the same way a room can feel messier before it can be properly organised.
Medication can sometimes support treatment if someone is also struggling with depression or another condition, but psychotherapy remains the central tool for personality-related patterns. The therapist's job is to keep the work grounded in daily life, not in abstract theory, so the conversation connects with what happens at home, at work, and in relationships.
Comorbidity and the Role of Medication
A common question is whether medicine can stand in for therapy. For borderline personality disorder, psychotherapy remains the main treatment, while medications do not have an approved indication for the condition and have not shown consistent results for its core symptoms (review).
Medication still has a place in care. It may be considered when depression, anxiety, sleep problems, or substance-related concerns are interfering with daily functioning, especially while a person is also starting psychotherapy. The role is supportive, helping with symptom relief so the person can stay engaged in treatment.
The broader evidence also helps set realistic expectations. In psychotherapy trials, the mean pre-post effect sizes within treatment were 1.11 for self-report measures and 1.29 for observational measures, which shows large change within treatment settings (American Journal of Psychiatry review). Earlier benchmark work found a 1.46 overall effect size for psychodynamic therapy and 1.00 for cognitive behaviour therapy, again supporting meaningful change rather than only short-term relief (meta-analysis).
If someone is also facing addiction, integrated care matters. In that situation, it can help to look at a service such as Empire Medical Wellness addiction care as one possible route for support alongside psychotherapy.
What this means in practice
Medication can reduce a symptom, while therapy is where new relationship habits and emotional skills are built. That is why the two are often discussed together but not treated as interchangeable.
Assessments are informational, not diagnostic, and that distinction matters when symptoms overlap. A person with depression, anxiety, trauma, or substance use concerns may need a broader evaluation before anyone tries to make sense of the full picture.
Prognosis and Recovery Evidence
Hope is easier to hold when it is grounded in evidence. One of the clearest findings in the literature is that structured psychotherapy can support recovery for a substantial share of people, with about 52% of those who stayed in therapy no longer meeting full diagnostic criteria after a mean of 1.3 years of treatment (AJP review).
How to read the numbers without getting lost in them
Effect sizes help show how much change took place, not just whether change happened. In the benchmark research, psychodynamic therapy showed a 1.46 overall effect size, with 1.08 for self-report outcomes and 1.79 for observer-rated outcomes, while cognitive behaviour therapy showed 1.00 overall (meta-analysis).
That matters because recovery is visible in two places at once, in how a person experiences themselves and in how patterns of behaviour look to others. The numbers do not mean everyone improves in the same way, and they do not erase dropout, pauses in treatment, or setbacks along the way.
The same review of psychotherapy trials estimated a recovery rate of 25.8% per year of therapy, compared with 3.7% in a naturalistic model of borderline personality disorder (AJP review). That gap helps explain why structured treatment is taken seriously.
What recovery can look like
Recovery does not mean becoming emotionless or never having hard days again. It can mean fewer crises, steadier relationships, more reliable work functioning, and a life that feels less ruled by fear, anger, or shame.

For readers in India, a practical next step is to start with an assessment, then book a consultation with a therapist who can explain their method clearly. Ask how they track change, what happens if sessions feel intense, and whether they use structured care.
The most honest message from the evidence is simple. Progress is real, recovery is possible, and structured therapy gives people a better chance to build new habits that last.
How to Choose a Therapist and Take Next Steps
Choosing a therapist involves practical considerations around stigma, cost, and access, and those realities vary by location. In India, some people begin with limited options nearby, while others may have many names to compare and still feel unsure about where to start. A careful first conversation often matters more than finding a perfect match immediately, because fit usually becomes clearer once the work begins.
What to look for
Look for someone who can explain their training, the type of therapy they use, and how they handle emotional difficulty. If they can describe goals, session structure, and follow-up clearly, that usually points to organised care rather than vague reassurance.
You can also ask whether they have experience with personality disorders, anxiety, depression, family conflict, or relationship distress. That question is practical, because many people first seek help for stress, burnout, or communication problems before they have any formal understanding of what's going on. A good therapist should be able to connect those everyday struggles to a treatment plan without making you feel judged.
DeTalks can be one starting point for finding therapists and using science-backed assessments, especially when someone wants information before booking a session. It works best as a bridge into care, not as a substitute for a clinical conversation.
A steady first step matters more than an urgent one.
Simple next steps
- Take an informational assessment if you want a clearer starting point.
- Shortlist a therapist who uses structured, evidence-based counselling.
- Ask about format, including individual sessions, group options, and expected length.
- Notice daily routines that support well-being, such as sleep, movement, and regular meals.
- Bring one real-life example to the first session, such as a fight, shutdown, or panic moment.
These steps do not guarantee a quick resolution, but they do create a workable path forward and do not guarantee that dropout or setbacks won't happen. They also make room for resilience, self-understanding, and a more compassionate relationship with yourself.
If you're trying to make sense of repeated patterns, DeTalks offers a place to explore therapists and science-backed assessments in one place. Visit DeTalks to take a thoughtful first step, compare support options, and find a path that fits your life.