You might have opened a report, discharge summary, insurance paper, or therapy note and seen something like F32.1 or F31. That small code can feel unsettling, especially if nobody explained what it means in plain language.
Seeking clarity about affective disorder ICD-10 is a common experience, and you're not alone. Many people in India first meet these terms in a hospital record, a psychiatry referral, or while trying to understand depression, anxiety, burnout, or sudden mood changes that are affecting work, sleep, or relationships.
These codes are not a judgement about your character. They are part of a shared medical language that clinicians use to record symptoms, organise care, and decide whether someone may need counselling, therapy, psychiatric review, or a broader health check.
This guide is informational, not diagnostic. It can help you understand the labels, ask better questions, and feel more confident about your next step toward well-being, resilience, and support.
Making Sense of Mental Health Codes
A common moment goes like this. You collect a prescription or lab file, glance at the corner, and notice F32.1. You search it online, find technical language, and end up more anxious than before.
That reaction makes sense. Clinical codes often look cold, while your experience is deeply human. You may be dealing with low mood, anxiety, workplace stress, exhaustion, or a feeling that life has lost colour. A code doesn't capture all of that, but it does help professionals communicate clearly.
Why these codes exist
The ICD-10 is an international classification system used to name and organise health conditions. In mental health, it helps doctors, therapists, hospitals, and administrative systems record what kind of problem is being seen.
In practice, that means your file may include a code so one professional's notes can make sense to another. If you want a plain-language companion for understanding how medical labels get translated across systems, this ICD-10 code mapping guide can be a useful reference.
A code is a shorthand for communication. It isn't the whole story of your emotional life.
What a code can and can't tell you
A code can suggest the general pattern a clinician is seeing. It can point to a depressive episode, a recurrent pattern, bipolar features, or a mood picture that still needs more assessment.
It can't tell you who you are, whether you'll recover, or what kind of support will help you most. That's why good care never stops at the code. It includes conversation, history, functioning, stressors, sleep, physical health, and your own goals for therapy or counselling.
If you've seen one of these labels, try not to read it as a final verdict. Read it as information you can use in a grounded, informed way.
What Are Affective Mood Disorders
The word affective relates to mood. So when clinicians talk about affective disorders, they mean conditions where a person's emotional state shifts in a way that significantly affects daily life, relationships, work, and well-being.
Mood naturally rises and falls. Everyone has difficult weeks, grief, stress before exams, or emotional strain during workplace conflict. An affective disorder is different because the mood change is more persistent, more intense, or part of a recognisable pattern that needs support.
Mood in human terms
For some people, the dominant experience is depression. They may feel slowed down, hopeless, numb, or unable to enjoy things that once mattered. Sleep, focus, appetite, and motivation may all be affected.
For others, the pattern includes heightened or unusually driven states as well. Energy may surge, sleep may drop, thoughts may race, and judgement may change. That pattern sits on the bipolar side of the mood spectrum.
Affective disorders can exist alongside anxiety, stress, and burnout. Someone may come to counselling because of irritability, panic, poor concentration, or workplace stress, then realise that a deeper mood pattern has also been present.
Why people often get confused
Many people mix up mood disorders with personality issues, stress reactions, or temporary emotional overwhelm. The lived experience can overlap, which is why assessment matters. If you want a helpful contrast between categories that are often confused, this insight on mental health conditions gives useful context.
Here are a few grounding ideas:
- Low mood isn't always a disorder. Sometimes it's a response to loss, pressure, conflict, or exhaustion.
- High energy isn't always wellness. In some cases, unusually high mood can signal a manic pattern rather than resilience.
- Support still matters either way. Whether the issue is stress, depression, anxiety, or an affective disorder, therapy and counselling can help you make sense of what you're living through.
Mental health labels work best when they reduce confusion, not when they increase shame.
The ICD-10 Framework for Mood Disorders F30 F39
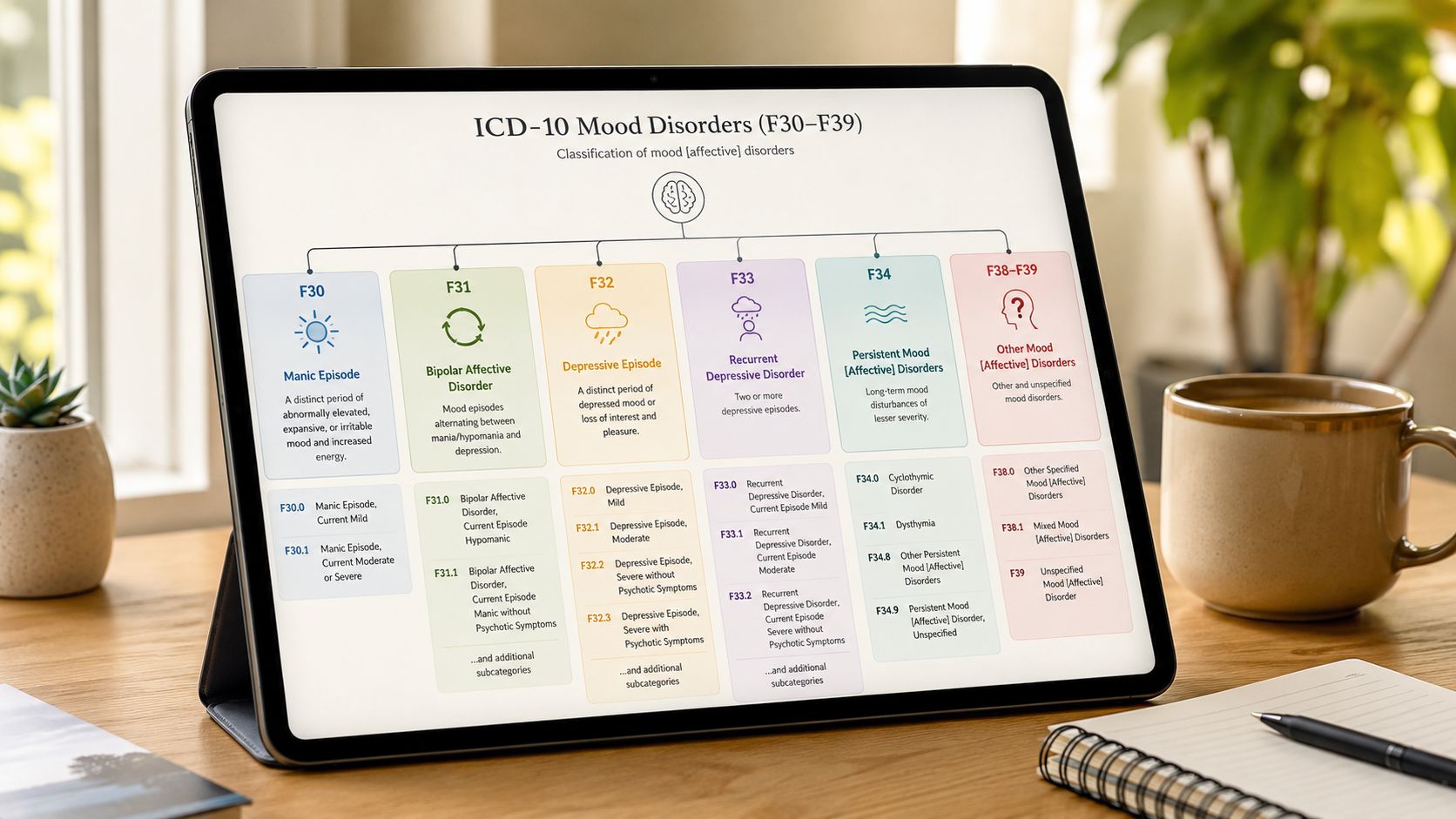
In ICD-10, mood disorders sit in a specific block: F30 to F39. This is the main framework used for affective disorders in ICD-10-based clinical and administrative work.
India-specific public health reporting has long used this F30-F39 block as the standard classification for affective disorders, including manic episode (F30), bipolar affective disorder (F31), depressive episodes (F32), recurrent depressive disorder (F33), persistent mood disorders (F34), other mood disorders (F38), and unspecified mood disorder (F39), which allows records to distinguish a one-time depressive episode from recurrent illness or bipolar disorder in clinical documentation and epidemiology (international ICD-10 grouping reference).

Quick map of the code family
| Code Block | Disorder Name | Brief Description |
|---|---|---|
| F30 | Manic episode | A period of unusually elevated or irritable mood with increased activity or energy |
| F31 | Bipolar affective disorder | A broader mood condition involving manic or related highs and depressive lows |
| F32 | Depressive episode | A current episode of depression |
| F33 | Recurrent depressive disorder | Depression that has occurred more than once over time |
| F34 | Persistent mood disorders | Longer-lasting mood patterns, often more chronic |
| F38 | Other mood disorders | Presentations that don't fit neatly into the main groups |
| F39 | Unspecified mood disorder | Mood symptoms are present, but the picture isn't yet specific enough |
Why this structure matters in real life
If you only saw the word "depression" on every file, it would be hard to know whether someone had a single low period, repeated episodes, or bipolar-related mood changes. The ICD-10 structure helps separate those patterns.
That matters because support may differ. A person with a first depressive episode may need one path. A person with recurring episodes may need a different long-term plan. A person with bipolar features may need especially careful review because treatment choices often depend on the full mood pattern, not only the current low phase.
For patients, the key takeaway is simple. The code family is a map. It doesn't replace a thoughtful conversation, but it gives your care team a common way to locate where your current experience might fit.
Detailed Look at Depressive Disorders F32 F33 F34
Affective disorder ICD-10 inquiries often focus on depression codes. This part of the system can feel technical, but the basic distinction is very human: is this a current episode, a repeated pattern, or a more persistent long-term low mood state?
F32 means a depressive episode
In ICD-10, depressive episode is coded as F32, with severity levels including mild F32.0, moderate F32.1, severe F32.2, and severe with psychotic symptoms F32.3. Recurrent depressive disorder is F33, and this coding structure helps clinical workflows in India map symptoms to standardised severity levels for triage between counselling, psychiatric review, and higher-acuity care (WHO ICD-10 browser for mood disorders).
Those severity labels can sound intimidating. In ordinary language, they help describe how much the depression is interfering with life.
- Mild often means the person is struggling but can still manage some daily tasks, though with effort.
- Moderate usually means work, study, relationships, and self-care are being affected more clearly.
- Severe suggests the impact is deeper, and functioning may be seriously disrupted.
- Severe with psychotic symptoms means the depressive state includes additional serious features that need specialist care.
F33 means the pattern has returned
F33 is used when depression isn't just a one-time episode. It points to a recurring pattern over time.
That distinction matters emotionally as well as clinically. If your low periods keep returning, it doesn't mean you've failed. It means your care may need to focus not only on symptom relief, but also on relapse awareness, resilience habits, stress management, and ongoing support.
Practical rule: If a depressive label appears on your record, ask whether the clinician is describing a current episode, a recurrent pattern, or a chronic low-grade mood condition.
Where F34 fits
F34 covers persistent mood disorders. In plain language, this points to mood difficulties that can last a long time and may feel woven into everyday life.
People with persistent low mood sometimes don't seek help quickly because they think, "This is just my personality," or "I've always been like this." But a long-standing pattern can still deserve therapy, counselling, and a careful look at sleep, stress, relationships, and self-worth.
A useful way to think about these codes is:
- F32 asks, "Are you in a depressive episode now?"
- F33 asks, "Has this happened repeatedly?"
- F34 asks, "Has low mood become more chronic or persistent?"
Understanding Bipolar and Manic Episodes F30 F31
Depression isn't the only part of the mood picture. Some people have periods of unusually heightened, expansive, or very irritable mood, along with more energy, less need for sleep, faster thinking, and a sense that everything is moving at high speed.
That is where F30 and F31 come in. These codes help clinicians distinguish a single manic episode from the broader pattern known as bipolar affective disorder.

F30 describes an episode
F30 is about a manic episode itself. The focus is the current or identified period of heightened mood and increased activity.
In everyday life, this might look like someone sleeping very little yet feeling unusually energised, talking much more than usual, making impulsive decisions, or feeling unusually powerful or unstoppable. Loved ones often notice the change before the person does.
F31 describes the wider condition
F31 refers to bipolar affective disorder. This is the broader pattern in which a person experiences episodes across different parts of the mood spectrum, including depressive periods and manic or related heightened states.
That distinction is important because a low mood within bipolar disorder is not the same as unipolar depression. Two people may both feel depressed in the present moment, but if one person also has a history of manic episodes, the overall clinical picture is different.
A side-by-side way to think about it
| Code | What it points to | Human meaning |
|---|---|---|
| F30 | Manic episode | "A high-energy mood episode is happening or has been identified" |
| F31 | Bipolar affective disorder | "The person's overall mood pattern includes both highs and lows" |
This is one reason detailed history-taking matters so much. If someone seeks help during a depressive phase, clinicians have to ask carefully about past periods of high mood, reduced sleep, unusual confidence, impulsive behaviour, or major shifts in activity.
A person can look depressed today and still have a bipolar pattern overall. The history matters as much as the current mood.
Whether stress, happiness, ambition, or productivity could be confused with mania is a very reasonable question. Healthy enthusiasm usually stays connected to judgement, rest, and stability. Mania often brings a stronger loss of balance, reduced insight, and consequences that others can see clearly.
Navigating Other and Unspecified Codes F38 F39
Some people's symptoms don't fit neatly into the main boxes. That doesn't mean the distress isn't real. It usually means the clinician is still working to understand the pattern more fully.
What F38 usually means
F38 covers other mood disorders. This can include mood presentations that are less typical or don't sit cleanly under the more familiar headings.
For patients, the important point is that "other" doesn't mean unimportant. It means the presentation is real but doesn't match the standard template in a simple way.
Why F39 can feel unsettling
F39 is unspecified mood disorder. People often see that word and worry that nothing clear is known. In reality, it can function as a holding code while more information is gathered.
A key issue is the boundary between F39 and medical mimics. F39 may be used when symptoms don't fit a more specific mood diagnosis, but this raises the risk of mislabelling depression-like symptoms that are related to thyroid disease, substance use, sleep disorders, medication effects, or acute stress, which is why an unspecified code may need broader reassessment rather than therapy alone (clinical discussion of F39 and diagnostic boundaries).
When an unspecified code should prompt questions
If you see F39, it can help to ask:
- Could a physical health issue be contributing? Thyroid problems, sleep disruption, medication effects, or other medical concerns can affect mood.
- Has acute stress changed the picture? Relationship conflict, grief, exams, financial pressure, or workplace stress can produce depression-like symptoms.
- Is more observation needed? Sometimes the pattern becomes clearer only over time.
Compassionate assessment is important. A person may need therapy and counselling, but they may also need a fuller medical review. F39 is often best understood as a sign to stay curious, not as the end of the conversation.
A Brief Glimpse at ICD-11 Changes
Mental health language doesn't stay frozen. Classification systems change because clinicians and researchers keep refining how they understand mood, functioning, and symptom patterns.

What changed in broad terms
ICD-10 grouped affective disorders under the familiar F30 to F39 structure. ICD-11 moves toward a more updated organisation of mood conditions, with clearer attention to symptom clusters, severity, and functional impact.
One important shift, noted in the earlier discussion of F39, is that ICD-11 places more emphasis on symptom clusters, severity, and functional impairment. That can help reduce overuse of vague labels and support more precise clinical thinking.
Why that matters for patients
This isn't something you need to memorise. The practical message is more reassuring than technical. Mental health care is trying to become more accurate, more useful, and more aligned with how people experience distress.
That matters if you've ever felt that a label seemed too broad or too vague. Updated systems try to improve clarity, especially when clinicians need to distinguish between depression, bipolar-related conditions, persistent low mood, or symptoms shaped by medical or psychosocial factors.
Better classification doesn't replace empathy. It gives empathy a clearer map to work with.
If your records still use ICD-10, that doesn't mean they're outdated in a harmful sense. It often reflects the coding system used in a given setting. What matters most is that the clinician listens well, reviews carefully, and explains the plan in terms you understand.
Your Next Steps Toward Well-being
Learning what a code means can be relieving, but it can also stir up new questions. You may recognise yourself in the description of depression, anxiety, workplace stress, or bipolar patterns. You may also feel unsure whether your symptoms reflect a mood disorder, burnout, grief, or something physical that needs checking.

A diagnosis code is only one part of the picture. Your sleep, stress load, support system, physical health, relationships, work environment, and coping style all matter too. So do your strengths, including resilience, compassion, creativity, and the ability to ask for help when something feels off.
Signs it's worth reaching out
You don't need to wait until things become unbearable. It may be time to seek support if mood changes are affecting everyday life in ways that feel hard to manage alone.
- Work and study are slipping. Concentration, motivation, attendance, or decision-making have become harder.
- Relationships feel strained. You feel more withdrawn, reactive, numb, or misunderstood.
- Daily care has become difficult. Sleep, appetite, hygiene, or routine are increasingly disrupted.
- You're worried by the pattern. Even if you can't name it, something feels persistently different.
Assessments can be useful here, but they are informational, not diagnostic. They can highlight patterns and help you decide whether to explore therapy, counselling, psychiatric support, or a medical check-up.
Choosing support with care
The right next step depends on what you're experiencing. Some people start with a counsellor or therapist. Some need a psychiatrist. Some benefit from both, especially when symptoms are intense, recurring, or mixed with sleep disruption, anxiety, or possible bipolar features.
If you're evaluating treatment options more broadly, including newer or highly specialised services, it's wise to use practical criteria such as credentials, safety standards, and clarity about indications. This guide on how to evaluate ketamine therapy clinics is a good example of the kind of careful, question-based approach that helps people make informed mental health decisions.
A short explainer can also help you pause and reflect before your next appointment.
A grounded path forward
In India, many people first seek help only after long periods of stress, anxiety, burnout, or silent depression. Starting earlier can make the process feel less overwhelming. Support doesn't have to begin with a dramatic crisis. It can begin with one honest conversation.
If you want a practical first step, platforms such as DeTalks let you browse mental health professionals in India, explore psychological assessments for insight, and decide whether therapy, counselling, self-help work, or psychiatric review fits your current needs.
What matters most is this. A code like F32, F33, F31, or F39 doesn't define your future. It gives you language, and language can help you move toward clarity, support, and a steadier sense of well-being.
If you're ready to turn confusion into a clearer next step, DeTalks offers a way to explore therapists, counsellors, and mental health assessments in one place. You can use it to understand what you're experiencing, find support that fits, and take one thoughtful step toward greater resilience and well-being.
Leave a Reply